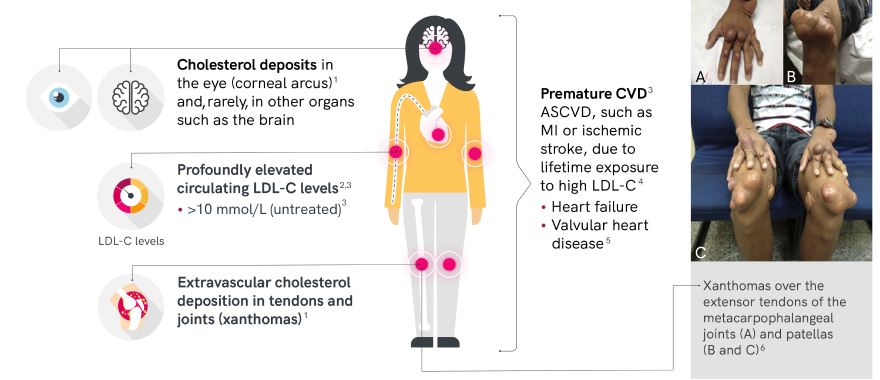
The clinical presentation of HoFH is variable and important to diagnose early
Both children and adults can present with a combination of the following signs according to the severity of the phenotype
© 1999-2023 BioMed Central Ltd.
© 2013-2023 J Am Coll Cardio.
ASCVD=atherosclerotic cardiovascular disease. CVD=cardiovascular disease. MI=myocardial infarction.
2023 ESC/EAS diagnostic criteria
- HoFH can be diagnosed using clinical and/or genotypic criteria recommended by the EAS Guidelines3
- HoFH should be suspected if untreated LDL-C levels are >10 mmol/L (> 400 mg/dL), requiring further evaluation including a detailed medical and family history and/or genetic testing3
| Clinical diagnostic criteria | Genotypic diagnostic criteria | |
|---|---|---|
| LDL-C >10 mmol/L* | Cutaneous or tendon xanthomas before age 10 years
and/or Untreated elevated LDL-C levels consistent with HeFH in both parents† |
Confirmation of two pathogenic variants in the LDLR, APOB, PCSK9, or LDLRAP1 genes or ≥2 such variants at different loci† |
LDLRAP=low-density lipoprotein receptor adapter protein 1. EAS=European Atherosclerosis Society. ESC=European Society of Cardiology.
LDLR=low-density lipoprotein receptor. APOB=apolipoprotein B. PCSK9=proprotein convertase subtilisin/kexin type 9.
* Lower LDL-C levels, especially in children or in treated patients, can be seen in genetically confirmed HoFH.
† In digenic form, one parent may have normal LDL-C levels and the other may have LDL-C levels consistent with HoFH.
‡ Bi-allelic pathogenic/likely pathogenic variants on different chromosomes at the LDLR, APOB, PCSK9, or LDLRAP1 genes or >2 such variants at different loci.
While genetic testing may aid diagnosis, HoFH may be present in patients without known FH-related mutations.7
Genetic testing is useful for risk stratification and, in the case of LDLR-deficient patients, may predict poor response to drug treatment.1
Importance of early and accurate diagnosis
HoFH is underdiagnosed and undertreated in the general population8,9
- There is a lack of awareness of HoFH among physicians10
- Many cases are not diagnosed in childhood, when atherosclerosis may be preventable11
- A significant proportion of patients are misdiagnosed following initial presentation, with HoFH often mistaken for HeFH3,12
The extent and duration of elevated total cholesterol, 90% of which is LDL-C in patients with HoFH, is generally proportional to the severity of atherosclerosis and all-cause and cardiovascular mortality, highlighting the need for prompt diagnosis and treatment initiation.13
Increasing risk of all-cause mortality with higher cholesterol level (on treatment)13
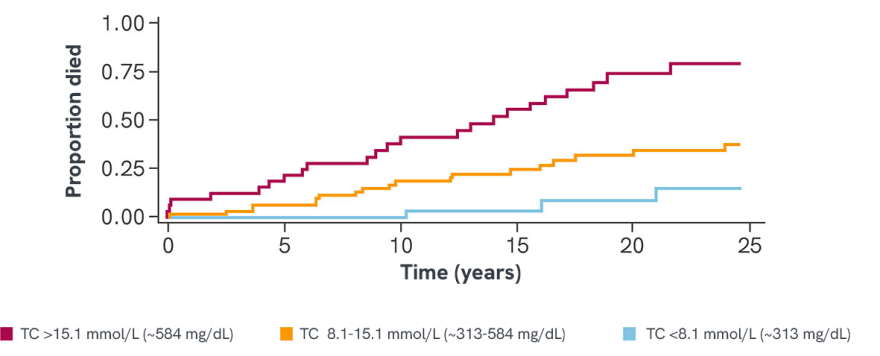
Adapted from Thompson, G R et al., 2018
TC=total cholesterol.
*Retrospective survey of lipid levels and clinical outcomes of 133 HoFH patients treated with a combination of lipid-lowering measures between 1990 and 2014 in South Africa and the UK
References
1. France M et al. Atherosclerosis. 2016;255:128-139. 2. Brunham L, et al. Can J Cardiol. 2018;34(12):1553-1563 3. Cuchel M et al. Eur Heart J. 2023;44(25):2277-2291. 4. Santos RD et al. Lancet Diabetes Endocrinol. 2016;4:850-861. 5. Fahed AC et al. Cholesterol. 2017;2017:3685265. 6. Rocha VZ et al. J Am Coll Cardiol. 2013;61:2193. 7. Ito MK, Watts GF. Drugs. 2015;75:1715-1724. 8. Nordestgaard BG et al. Eur Heart J. 2013;34:3478-3490. 9. Baum SJ et al. J Clin Lipidol. 2014:542-549. 10. Bouhairie VE, Goldberg AC. Cardiol Clin. 2015;33:169-179. 11. Alonso R et al. J Clin Lipidol. 2016;10:953-961. 12. Hemphill L et al. J Gen Intern Med. 2020;35:2225-2227. 13. Thompson GR et al. Eur Heart J. 2018;39:1162-1168.